
Axial - Observations #40
Life sciences reflections

More well thought out work can be found at — https://axial.substack.com/
Axial partners with great founders and inventors. We invest in early-stage life sciences companies often when they are no more than an idea. We are fanatical about helping the rare inventor who is compelled to build their own enduring business. If you or someone you know has a great idea or company in life sciences, Axial would be excited to get to know you and possibly invest in your vision and company . We are excited to be in business with you - email us at info@axialvc.com
Observations #40
A set of ideas and observations from a week’s worth of work analyzing businesses and technologies.
Voice in healthcare
Everything in healthcare from diagnostics to prescriptions starts with a conversation between a patient and their doctor. Given the massive improvements in voice recognition and transcription technology, with the best example in Alexa, bringing these tools to healthcare can help patients remember the conversations they have with their doctor, help physicians save time, and reduce billing errors.
The two leading companies in the field are Abridge and Suki. Both are building similar products to track and translate the conversations between a patient and doctor into actionable results, but Abridge is focused on acquiring consumers and Suki on healthcare providers.
For the patient:
A voice recording product can help them control part of their own health records. They could share their conversations with doctors with other clinicians and care providers.
They more easily remember details from their conversations. Like what medications they need to take and why. Their diagnoses and more.
Increasing compliance rates (i.e. filling their prescriptions, follow-ups)
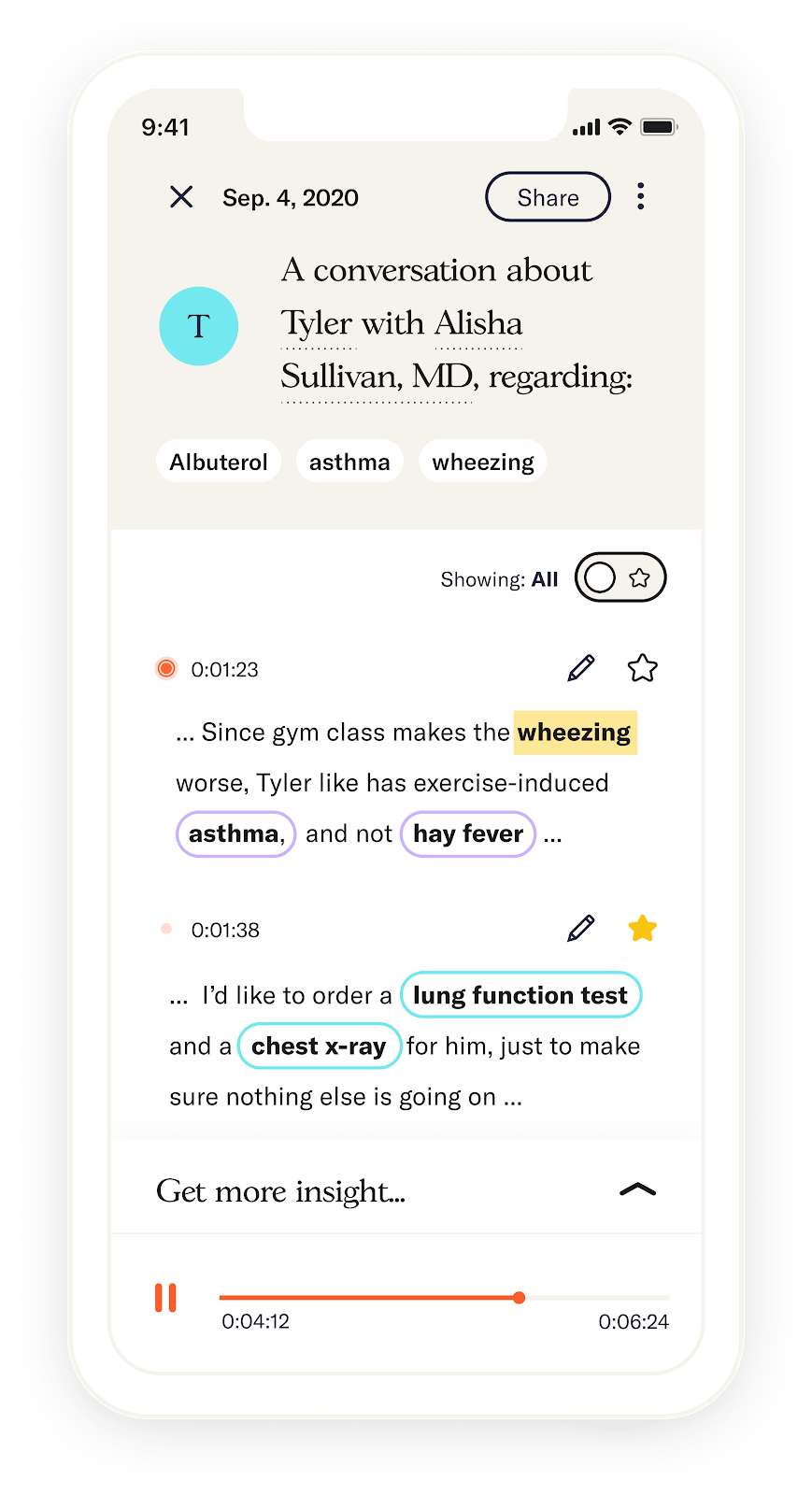
Source: Abridge
For the doctor:
Reduce the time they spending taking medical notes and increase their time with patients by transcribing a conversation into an EHR
Help retrieve certain medical information like charts more easily
Condense a conversation they have with a patient into an actionable plan
Integrate with other service providers like PBMs to automatically prescribe a medicine to their patient
Increase the quality of treatment plans and information on their patient, to reduce claim denials
Building voice products in healthcare has the potential to introduce virtual assistants to the exam room. In combination with machine learning, these products can become personalized to both the patient and doctor. Technical challenges remain to define the large universe of medical terms and implement algorithms that can recognize patient-relevant words while accommodating for differing qualities of microphones in the exam room. Privacy and security is also incredibly important.
N-of-1 trials
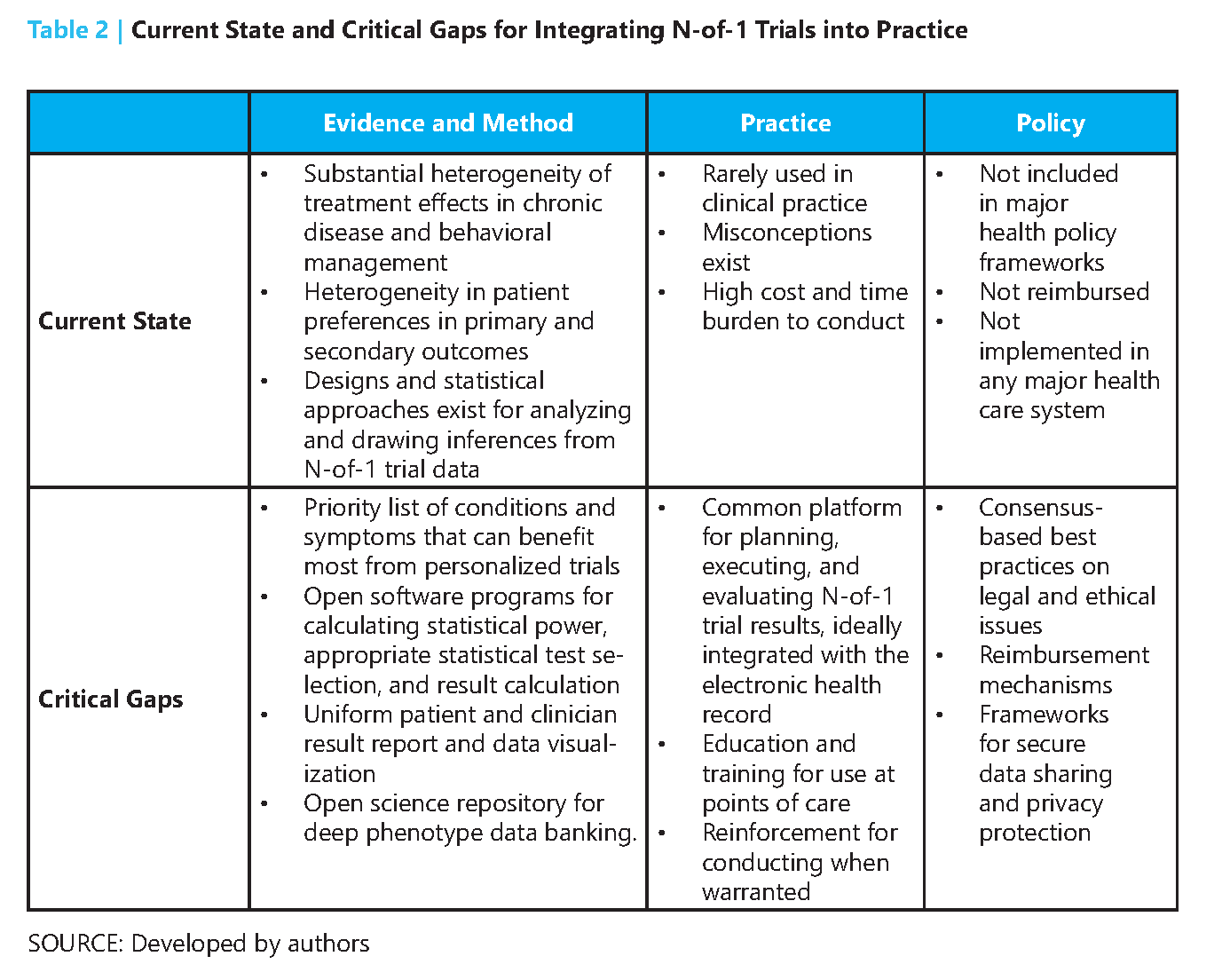
N-of-1 trials focus on understanding the effects of various interventions for an individual patient. In 1986, a group out of McMaster University published the first paper defining N-of-1 trials inspired by a drug trial for asthma - https://www.nejm.org/doi/pdf/10.1056/NEJM198604033141406 In this type of trial, a patient alternates between taking a drug and placebo. These treatments can be sequenced in various ways to establish the effects of the drug. After the trial, statistical analysis tools can be used to determine the efficacy of the drug and the one trial can be aggregated with other N-of-1 trials to infer the drug’s efficacy across a population.
N-of-1 trials are valuable for their ability to capture intra-individual variation. Other trial designs are good for inter-individual diversity and meet their limitations where patient responses to an intervention have high variation. N-of-1 become useful in situations where a randomized clinical trial (RCT) cannot address:
Diseases with low prevalence (i.e. rare diseases)
Diseases with large response variability (i.e. chronic pain)
Patients who have been on long-term treatment regimens
Patients who are medical outliers
In short, N-of-1 trials can make drug development for rare diseases feasible where thousands have no approved medicine. Moreover, N-of-1 trials can act as an early signal on where to engage in a costly RCT and identify predictors of response beforehand. Ensuring trial quality across patients and comprehensive reporting can help N-of-1 trials to gain more acceptance from the medical community. Two large opportunities are to bring the power of antisense oligonucleotides (ASO) to N-of-1 trials (invest upfront and costs go down overtime) and build better software/data tools to capture data from these trials and put them into an EHR so results can be aggregated and analyzed with confidence by clinicians.
Patient-driven drug development
Early-stage drug development, particularly in rare diseases, have high risks of failure or are too small of markets to attract substantial venture capital. As a result, foundations and patients have been groups that fill in this gap. With better tools to build communities and precedents set, patients can have an increasingly powerful role in starting new companies and sparking the development of medicines for their disease. Opportunities in the field are:
Building a network of patients and their data - using a Flatiron-type of model to collect natural history of patients, especially those with rare diseases.
Aggregating foundations - to provide resources like patient support, help with trial recruitment, and understanding of new and emerging treatments
Hand off to industry - foundations and patient groups are experts in their disease and help industry understand how the field is developing. The Parker Institute for Cancer Immunotherapy does a great job here.
Minimizing conflicts-of-interest - foundations and companies need to find a balance to manage actual and perceived conflicts-of-interest especially if foundations take equity stakes in the companies
Monetizing equity and royalties - finding efficient pathways for foundations and patient groups to profit from their early investment in order to reinvest the capital into their non-profit activities. The Cystic Fibrosis Foundation and Aurora Biosciences, which was acquired by Vertex and led to the approval of Kalydeco in cystic fibrosis is the best example of this.
Translating research into products - many diseases, rare diseases mainly, do not have an established scientific understanding. As a result, foundations have to fill in the gap and invest in basic research to set up drug development for these diseases down the line.
The best example so far of patient-driven drug development is the Cystic Fibrosis Foundation (CFF) and Kalydeco. CFF’s mission is to cure cystic fibrosis (CF), a rare disease that affects ~40K people in the US. The CFF was formed in 1955 and spent decades funding basic research in CF and building a database of patients. In 2000, the foundation invested $30M in Aurora Biosciences to develop new medicines for CF targeting a mutation discovered by labs in the 1980s funded by the CFF. Vertex acquired Aurora in 2001 and the CFF maintained their drug development agreement leading to the approval for Kalydeco in 2012. In 1980, the median age of survival for a CF patient was 18 and by 2016 that age of survival increased to well above 45 years old. Inspiring work by the CFF and serves as a case study for the power of patient-driven drug development. The foundation continues to support the development of new medicines with Orkambi (a combination of Kalydeco and Lumacaftor) recently approved for CF and ensure patient access to these transformative drugs.
Other examples of successful patient-driven drug development are LifeArc and Keytruda along with the Juvenile Diabetes Research Foundation, Emerson Collective, PICI, and the Michael J. Fox Foundation. These groups have the power to lower the barriers for drug development in particular diseases by providing patients, scientific expertise, and capital.
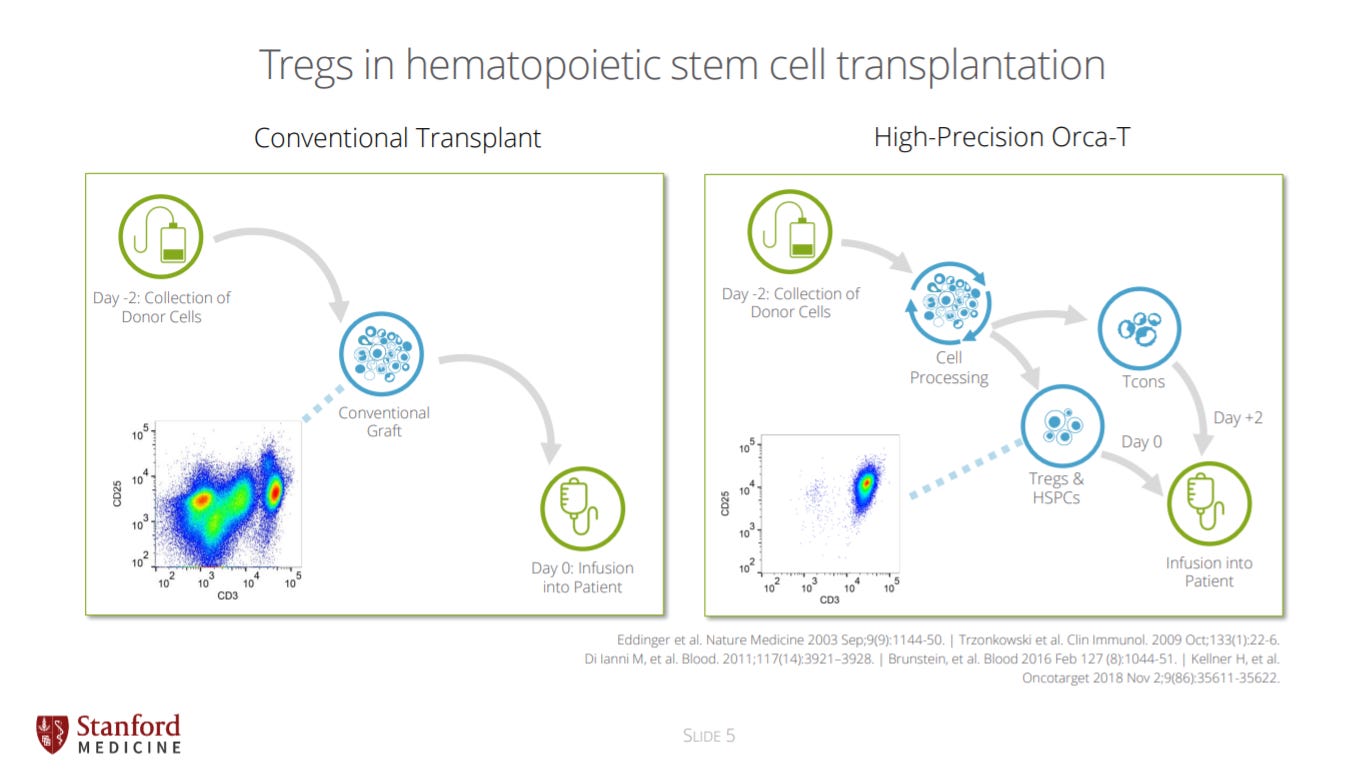
A revolution for BMTs
Orca Bio published recent data at ASH https://orcabio.com/ASH_2020_Orca_Bio.pdf after years of work to show massive reductions in GvHD. Congratulations to Ivan, Nate, and everyone on the team. The best is yet to come.
What is Life? cont.
In Chapter 6 (Order, Disorder, and Entropy) of What is Life?, Schrödinger discusses the interplay of order and disorder for life. In short, he concludes a major feature of life is its ability to export entropy. Life has order but is in an environment with increasing entropy. So in order to resist the natural tendency of its environment, life must generate negative entropy to maintain its structure:
“What is the characteristic feature of life? When is a piece of matter said to be alive? When it goes on 'doing something', moving, exchanging material with its environment, and so forth, and that for a much longer period than we would expect an inanimate piece of matter to 'keep going' under similar circumstances. When a system that is not alive is isolated or placed in a uniform environment, all motion usually comes to a standstill very soon as a result of various kinds of friction; differences of electric or chemical potential are equalized, substances which tend to form a chemical compound do so, temperature becomes uniform by heat conduction. After that the whole system fades away into a dead, inert lump of matter. A permanent state is reached, in which no observable events occur. The physicist calls this the state”
“From Delbruck's general picture of the hereditary substance it emerges that living matter, while not eluding the 'laws of physics' as established up to date, is likely to involve 'other laws of physics' hitherto unknown, which, however, once they have been revealed, will form just as integral a part of this science as the former.”
“What is the characteristic feature of life? When is a piece of matter said to be alive? When it goes on 'doing something', moving, exchanging material with its environment, and so forth, and that for a much longer period than we would expect an inanimate piece of matter to 'keep going' under similar circumstances. When a system that is not alive is isolated or placed in a uniform environment, all motion usually comes to a standstill very soon as a result of various kinds of friction; differences of electric or chemical potential are equalized, substances which tend to form a chemical compound do so, temperature becomes uniform by heat conduction. After that the whole system fades away into a dead, inert lump of matter. A permanent state is reached, in which no observable events occur. The physicist calls this the state”
“What then is that precious something contained in our food which keeps us from death? That is easily answered. Every process, event, happening - call it what you will; in a word, everything that is going on in Nature means an increase of the entropy of the part of the world where it is going on. Thus a living organism continually increases its entropy - or, as you may say, produces positive entropy - and thus tends to approach the dangerous state of maximum entropy, which is death. It can only keep aloof from it, i.e. alive, by continually drawing from its environment negative entropy - which is something very positive as we shall immediately see. What an organism feeds upon is negative entropy. Or, to put it less paradoxically, the essential thing in metabolism is that the organism succeeds in freeing itself from all the entropy it cannot help producing while alive.”